
Anaemia is a common feature of CKD associated with poor outcomes. The current management of patients with anaemia in CKD is controversial, with recent clinical trials demonstrating increased morbidity and mortality related to erythropoiesis-stimulating agents.1
 Chronic kidney disease (CKD) is a leading global public health challenge with an estimated prevalence of 13.4% (11.7-15.1%) worldwide.2 In India, deaths from CKD increased from 0.59 million in 1990 to 1.18 million in 2016. Andhra Pradesh, Odisha, Maharashtra, Goa, and Tamil Nadu reported an exceptionally high burden.3 The global estimated prevalence of end-stage renal disease (ESRD) patients needing renal replacement therapy is between 4.902 and 7.083 million.2 In India, owing to its growing population and ongoing demographic transitions, the rising incidence of CKD will likely constitute significant problems for both healthcare and the economy in the years to come.4 The age-adjusted incidence rate of ESRD in India is estimated to be 229 per million population, with >100,000 new patients entering renal replacement programs annually in India. However, only 10% of the Indian ESRD patients receive renal replacement therapy, owing to inadequate resources. Therefore, community-based screening programs like Screening and Early Evaluation of Kidney Disease Project (SEEK) must help early detection of kidney disease and generate data to determine the prevalence and risk factors for CKD in India.5 The increasing prevalence of diabetes mellitus, hypertension, obesity, and aging contribute significantly to the global surge in CKD, and in many countries, CKD is now among the top five causes of death.2,4
Chronic kidney disease (CKD) is a leading global public health challenge with an estimated prevalence of 13.4% (11.7-15.1%) worldwide.2 In India, deaths from CKD increased from 0.59 million in 1990 to 1.18 million in 2016. Andhra Pradesh, Odisha, Maharashtra, Goa, and Tamil Nadu reported an exceptionally high burden.3 The global estimated prevalence of end-stage renal disease (ESRD) patients needing renal replacement therapy is between 4.902 and 7.083 million.2 In India, owing to its growing population and ongoing demographic transitions, the rising incidence of CKD will likely constitute significant problems for both healthcare and the economy in the years to come.4 The age-adjusted incidence rate of ESRD in India is estimated to be 229 per million population, with >100,000 new patients entering renal replacement programs annually in India. However, only 10% of the Indian ESRD patients receive renal replacement therapy, owing to inadequate resources. Therefore, community-based screening programs like Screening and Early Evaluation of Kidney Disease Project (SEEK) must help early detection of kidney disease and generate data to determine the prevalence and risk factors for CKD in India.5 The increasing prevalence of diabetes mellitus, hypertension, obesity, and aging contribute significantly to the global surge in CKD, and in many countries, CKD is now among the top five causes of death.2,4
Kidney disease-related anaemia, a common complication of ESRD, correlates well with exalted morbidity, mortality, and healthcare costs. Anaemia begins to manifest when eGFR falls below 60 mL/min/1.73 m2 (Stage 3).6 The National Health and Nutrition Examination Survey (NHANES) analysis pronounced that 15.4% (~4.8 million people) had anaemia of CKD, and prevalence of anaemia was 17.4%, 50.3%, and 53.4% in CKD Stages 3, 4, and 5, respectively.7 India has the highest prevalence of anaemia globally at 39.86% which increased from 66.6% at Stage 3 to 94.7% at Stage 5.8,9
For patients worldwide with CKD who are not undergoing dialysis, a delayed referral to nephrologists and concerns regarding the safety of erythropoiesis-stimulating agents (ESAs) could let anaemia remain undertreated for a prolonged period.10 Increased healthcare costs and worsening quality of life are the other issues of concern in India. Anaemia is associated with an increased risk of cardiovascular comorbidities, prolonged hospital stays, reduced quality of life, and activity impairment.11
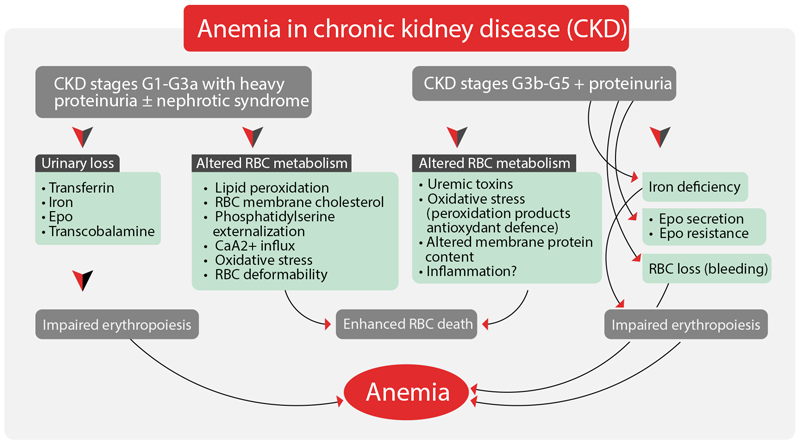
1. CKD Induced Anaemia: Pathophysiology Figure 1: HIF-PHIs Improve Efficient Erythropoiesis by Inhibition of Prolyl Hydroxylase 11
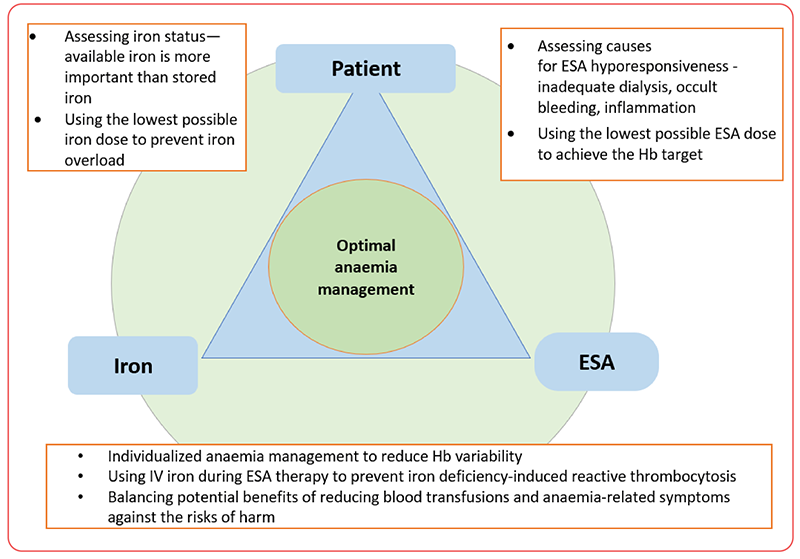
2. Management of CKD Induced Anaemia: Current Treatment Strategies Oral or intravenous (IV) iron, erythropoiesis-stimulating agents (ESAs) (IV and subcutaneous), and red blood cell (RBC) transfusion comprise the current standard of care for anaemia of CKD, each of which has inherent problems and varying effectiveness.
Figure 2: Interaction of Patient, Erythropoiesis-Stimulating Agent (ESA), and Iron in the Management of Anaemia (in CKD)12
REFERENCES: